Chiropractic SOAP Notes: Complete Guide, Examples, Templates & Best Practices
25.06.26
How much time do you spend documenting patient visits, and how confident are you that your notes would hold up during an audit or insurance review?
Chiropractic SOAP notes do much more than document what happened during an appointment. They help chiropractors track patient progress, support clinical decisions, communicate treatment plans, and maintain accurate records for compliance and insurance purposes.
Yet, many chiropractors still struggle to balance thorough documentation with the demands of a busy schedule. To help you avoid this, we’ll break down the structure of chiropractic SOAP notes, review real-world examples, and share proven tips for smoother administrative work.
Standing for Subjective, Objective, Assessment, and Plan, SOAP notes are a standardized method of documenting patient visits across various practices. This format helps chiropractors organize clinical information in a clear, consistent way while creating a detailed record of the patient’s condition, treatment, and progress.
The SOAP framework has been widely used across healthcare for decades because it supports continuity of care, clinical decision-making, and accurate documentation. For chiropractors, this type of progress note also plays an important role in insurance claims, compliance requirements, and tracking patient outcomes over time.
Each section serves a specific purpose:
Subjective: What the patient reports about their symptoms, pain levels, and functional limitations.
Objective: Measurable findings gathered during the examination, such as range of motion, posture, orthopedic tests, or palpation results.
Assessment: The chiropractor’s clinical interpretation of the patient’s condition and response to treatment.
Plan: The next steps, including adjustments, therapies, home exercises, and follow-up recommendations.
Keeping a consistent approach to documenting patient records, chiropractic SOAP notes create a complete picture of the patient’s care journey while making it easier to evaluate progress from one visit to the next.
SOAP Notes vs Narrative Notes
SOAP notes and narrative notes are both used to document patient encounters, but they differ significantly in structure and usability.
Feature
SOAP Notes
Narrative Notes
Structure
Organized into Subjective, Objective, Assessment, and Plan sections
Free-form written summary of the visit
Consistency
Standardized format used across visits
Varies by practitioner and writing style
Ease of Review
Information is easy to locate and scan
Important details may be buried in paragraphs
Progress Tracking
Makes it simple to compare patient progress over time
Progress can be harder to identify quickly
Insurance & Audits
Supports clear documentation for claims and compliance
May require additional clarification or review
Efficiency
Faster to complete when using templates or digital documentation
Can take longer to write and review
Best For
Routine clinical documentation and ongoing patient care
While narrative notes can be useful for documenting unique or complex situations, most chiropractors rely on the SOAP note-taking because it provides a consistent approach and helps document the details faster.
Besides satisfying documentation requirements, good SOAP notes create a reliable clinical record that supports patient care, protects your chiropractic practice, and makes day-to-day operations more efficient.
Whether you’re seeing 10 patients a day or managing a busy schedule with dozens of appointments, well-written SOAP notes help you spend less time trying to remember previous visits and more time making informed treatment decisions.
They also help you to:
Improve Continuity of Care
Every patient visit builds on the previous one. Clear SOAP notes make it easy to understand how symptoms have changed, which treatments have been effective, and what the next steps should be.
For example, if a patient has been receiving care for chronic lower back pain over several weeks, your previous notes should quickly show changes in pain levels, range of motion, treatment response, and home exercise compliance. This allows you to adjust the care plan based on objective progress rather than memory alone.
Consistent documentation is equally valuable when multiple practitioners work within the same clinic. Any chiropractor reviewing the patient’s record should be able to understand the case without needing additional explanation.
Support Clinical Decision-Making
SOAP notes guide future treatment decisions. When documenting objective findings and the patient’s reported symptoms, you can identify trends that may otherwise go unnoticed.
Over time, these records also make it easier to evaluate whether a treatment plan is working or whether modifications are needed.
Help Defend Against Audits and Claims
Unfortunately, there may be times when you’ll need to justify the care you provided to a legal representative. In those cases, SOAP notes act as the strongest evidence of your clinical decisions and examination findings.
Missing objective findings, incomplete treatment plans, or vague assessments can make it difficult to justify services after the fact. Taking an extra minute to document clearly today can save hours of stress if your records are ever questioned.
Reduce Documentation Errors
Busy clinics leave little room for paperwork mistakes. Rushed notes, incomplete records, or copy-and-paste documentation can lead to inaccuracies that affect patient care and create unnecessary administrative work later.
Using a standardized SOAP note format helps ensure that every visit includes the essential clinical information. Digital templates can further improve consistency by prompting chiropractors to document the same key elements during each appointment.
For practices seeing a high volume of patients, even small improvements in documentation efficiency can add up significantly over time. Solutions like Ruana help streamline this process with structured SOAP note workflows designed specifically for chiropractic practices, making it easier to create complete, consistent records while spending less time on documentation.
Simplify Insurance Documentation
Accurate documentation makes the insurance process smoother for both chiropractors and administrative staff.
When SOAP notes clearly describe the patient’s condition, examination findings, treatment performed, and ongoing progress, it’s much easier to support claims and prepare the documentation insurers may request.
Many modern chiropractic practices also reduce duplicate work by using practice management software that connects SOAP notes with patient records, scheduling, billing, and documentation. Instead of switching between multiple systems, practitioners can keep everything organized in one workflow while maintaining consistent records throughout the patient’s care journey.
Every chiropractic charting follows the same four-part structure, but the quality of your documentation depends on what you include in each section. The goal is to create a clear, concise record that accurately reflects the patient’s condition, your clinical findings, and the care provided during the visit.
Here’s what each part of a chiropractic SOAP note should contain.
Subjective (S)
The Subjective section captures information reported directly by the patient.
Include:
Chief complaint
Pain location and severity (for example, using a pain scale)
Changes in symptoms since the previous visit
Functional limitations or activities affected
Patient-reported response to previous treatment
Relevant updates to medical history or medications, when applicable
Objective (O)
The Objective section records measurable findings from your examination.
Include:
Posture and gait observations
Range of motion findings
Palpation findings
Orthopedic and neurological test results
Muscle strength or flexibility assessments
Vital signs, when appropriate
Areas adjusted or treated during the visit
Assessment (A)
The Assessment section is your clinical evaluation based on the patient’s symptoms and examination findings.
Include:
Clinical impression or diagnosis
Patient’s progress since the previous visit
Response to current treatment plan
Changes in functional status
Whether the current treatment plan remains appropriate or requires modification
Plan (P)
The Plan outlines what happens next and provides a roadmap for ongoing care.
Include:
Chiropractic adjustments performed
Additional therapies or modalities provided
Home exercises or self-care recommendations
Lifestyle or ergonomic advice, when relevant
Follow-up appointment schedule
Goals for the next phase of treatment
Keeping each section focused and consistent makes SOAP notes easier to review, improves communication across the practice, and creates a reliable record of the patient’s progress throughout their course of care.
Free Chiropractic SOAP Note Examples by Condition
While every patient presents differently, following a consistent SOAP format makes documentation easier to write, review, and update over the course of treatment.
The examples below are inspired by real-world clinical workflows and the everyday documentation practices we’ve developed in our own chiropractic office. While they have been simplified for educational purposes and don’t represent actual patient records, they reflect the structure, level of detail, and clinical thinking that help practitioners create clear, accurate, and efficient SOAP notes.
💡Use them as a practical reference when building documentation habits that are both thorough and time-efficient.
Lumbar Segmental Dysfunction / Lower Back Pain SOAP Note Example
Patient: [Patient Name]
Date of Service: [Date]
Provider: [Provider Name], D.C.
Visit Type: Initial chiropractic visit
Chief Complaint: Lower back pain
S — Subjective
Patient presents with lower back pain that began three days ago after lifting heavy boxes. Patient reports dull, aching pain localized to the lower lumbar region, greater on the right side, and points to the L4-L5 / right sacroiliac region as the primary area of discomfort. Pain is rated 6/10 today.
Patient states the pain began after bending forward and lifting heavy boxes. Pain increases with prolonged sitting, bending forward, lifting, and moving from sitting to standing. Patient reports difficulty sitting longer than approximately 20–30 minutes and is avoiding normal lifting activities due to pain. Symptoms are temporarily improved with rest and position changes.
Patient denies pain radiating into the lower extremities, numbness, tingling, weakness, bowel or bladder changes, saddle anesthesia, fever, unexplained weight loss, or other new symptoms. Patient reports no prior treatment for this episode.
O — Objective
Inspection reveals guarded lumbar movement during the sit-to-stand transition. Lumbar flexion is reduced approximately 20% with pain at the end range. Lumbar extension and right lateral flexion are mildly restricted and reproduce right-sided lower lumbar discomfort.
Static and motion palpation reveal segmental restriction / joint dysfunction at L4-L5 and the right sacroiliac region. Palpation over the L4-L5 and right SI region reproduces localized tenderness. Hypertonicity and tenderness are present in the lumbar paraspinal musculature, greater on the right.
Kemp’s test is positive on the right for localized lower lumbar pain without radicular symptoms. Straight leg raise is negative bilaterally. Lower extremity motor, sensory, and reflex screening are within normal limits. No neurological deficits observed.
A — Assessment
Diagnosis: Acute lumbar sprain/strain with associated lumbar segmental dysfunction and lumbar paraspinal muscle spasm/hypertonicity.
Findings are consistent with acute mechanical lower back pain following a lifting injury. The clinical presentation supports lumbar sprain/strain with segmental joint dysfunction at L4-L5 and associated right-sided lumbar paraspinal hypertonicity. Supporting findings include lower back pain rated 6/10, reduced lumbar flexion, painful lumbar extension and right lateral flexion, localized tenderness over the L4-L5 / right SI region, positive right Kemp’s test for localized lumbar pain, and functional limitations with sitting, bending, lifting, and sit-to-stand movement.
No current clinical findings suggest lumbar radiculopathy or neurological deficit. Straight leg raise is negative bilaterally, and lower extremity motor, sensory, and reflex screening are within normal limits. Red flag screening is negative based on patient history and today’s examination.
Conservative chiropractic care is indicated to reduce pain, improve lumbar range of motion, address lumbar segmental dysfunction, decrease paraspinal hypertonicity, and improve tolerance with activities of daily living. Prognosis is good with patient compliance, activity modification, and completion of the recommended treatment plan.
P — Plan / Procedures
Initial findings and the recommended treatment plan were reviewed with the patient. Patient consented to chiropractic treatment. Chiropractic manipulative therapy was performed to the lumbar spine and right sacroiliac region using [Diversified / Drop Table / Flexion-Distraction / Activator / other technique], with treatment directed to restricted segments at L4-L5 and the right SI region. Soft tissue therapy was performed on the lumbar paraspinal musculature, with greater emphasis on the right side.
Patient tolerated treatment well with no adverse reaction reported during or immediately after care. Post-treatment, the patient reported a mild reduction in discomfort and improved ease of lumbar movement.
Home care instructions were reviewed, including gentle lumbar mobility exercises, short walks as tolerated, frequent position changes, and avoidance of heavy lifting, repeated bending, or prolonged sitting for the next 48 hours. Patient was advised to stop any activity that increases symptoms.
The recommended treatment plan is 6 chiropractic sessions at a frequency of 2 visits per week for 3 weeks. Re-examination will be performed after the 6th visit to reassess pain level, lumbar range of motion, orthopedic findings, palpation findings, functional tolerance, response to care, and need for further treatment.
Patient was advised to seek urgent medical care if new or worsening symptoms develop, including radiating leg pain, numbness, weakness, bowel or bladder changes, saddle anesthesia, fever, or severe unrelenting pain.
👉Why this works
This note combines the patient’s reported symptoms with measurable examination findings and clearly explains the clinical reasoning behind the treatment plan. It also establishes a baseline that makes future progress easy to evaluate.
Cervical Segmental Dysfunction / Neck Pain SOAP Note Example
Patient: [Patient Name]
Date of Service: [Date]
Provider: [Provider Name], D.C.
Visit Type: Initial chiropractic visit
Chief Complaint: Right-sided neck pain
S— Subjective
Patient presents with right-sided neck pain rated 5/10 that began after several days of prolonged computer work. Patient describes the pain as stiffness and tightness in the right cervical region, with discomfort most noticeable in the morning and when turning the head to the right.
They report that symptoms increase with prolonged sitting, computer work, poor posture, and right cervical rotation. The patient states the pain interferes with turning the head while driving, maintaining comfortable posture at the computer, and performing normal work activities without frequent position changes. Symptoms are temporarily improved with rest, position changes, and gentle stretching.
Patient denies pain radiating into the upper extremities, numbness, tingling, weakness, dizziness, visual changes, headache worsening with exertion, bowel or bladder changes, fever, unexplained weight loss, recent trauma, or other new symptoms. Patient reports no prior treatment for this episode.
O — Objective
Inspection reveals mild forward head posture and guarded cervical movement with right rotation. Cervical rotation to the right is restricted by approximately 15 degrees and reproduces right-sided cervical discomfort. Cervical extension and right lateral flexion are mildly restricted, with tightness noted at end range.
Static and motion palpation reveal segmental restriction / joint dysfunction at the C5-C6 region, greater on the right. Palpation over the right C5-C6 region reproduces localized tenderness. Increased tone, tightness, and tenderness are noted in the right upper trapezius and right levator scapulae musculature.
Cervical compression is negative for radicular symptoms. Foraminal compression / Spurling’s test is negative for upper extremity referral. Upper extremity motor, sensory, and reflex screening are within normal limits. No neurological deficits observed.
A — Assessment
Diagnoses:
M99.01 — Segmental and somatic dysfunction of cervical region
M54.2 — Cervicalgia
Findings are consistent with acute mechanical neck pain associated with cervical segmental dysfunction and postural strain following prolonged computer work. Clinical findings support cervical joint dysfunction at C5-C6 with associated right upper trapezius and levator scapulae hypertonicity.
Patient presents with neck pain rated 5/10, restricted right cervical rotation, mild limitation with extension and right lateral flexion, localized tenderness over the C5-C6 region, increased muscle tone in the right upper trapezius and levator scapulae, and functional limitation with computer work, posture tolerance, and turning the head to the right.
No current clinical findings suggest cervical radiculopathy or neurological deficit. Red flag screening is negative based on patient history and today’s examination.
Conservative chiropractic care is indicated to reduce pain, improve cervical range of motion, address cervical segmental dysfunction, decrease muscle hypertonicity, and improve tolerance with work and daily activities. Prognosis is good with patient compliance, ergonomic modification, and completion of the recommended treatment plan.
P — Plan / Procedures
Initial findings and the recommended treatment plan were reviewed with the patient. Patient consented to chiropractic treatment.
Chiropractic manipulative therapy was performed on the cervical spine using [Diversified / Drop Table / Activator / other technique], with treatment directed to restricted segments at C5-C6. Myofascial release / soft tissue therapy was performed on the right upper trapezius and right levator scapulae musculature.
Patient tolerated treatment well with no adverse reaction reported during or immediately after care. Post-treatment, the patient reported a mild reduction in stiffness and improved ease of right cervical rotation.
Workstation ergonomics were reviewed, including monitor height, chair position, keyboard/mouse placement, posture breaks, and avoiding prolonged static head-forward posture. Home care instructions were reviewed, including gentle cervical mobility exercises, postural breaks during computer work, and avoidance of prolonged sitting without movement.
The recommended treatment plan is 6 chiropractic sessions at a frequency of 2 visits per week for 3 weeks. Re-examination will be performed after the 6th visit to reassess pain level, cervical range of motion, orthopedic findings, palpation findings, work/activity tolerance, response to care, and need for further treatment.
Patient was advised to seek urgent medical care if new or worsening symptoms develop, including radiating arm pain, numbness, tingling, weakness, dizziness, visual changes, severe headache, fever, or severe unrelenting pain.
👉Why this works
The note identifies the likely contributing factors, documents objective restrictions, and includes practical recommendations that support the overall treatment plan rather than focusing solely on the adjustment.
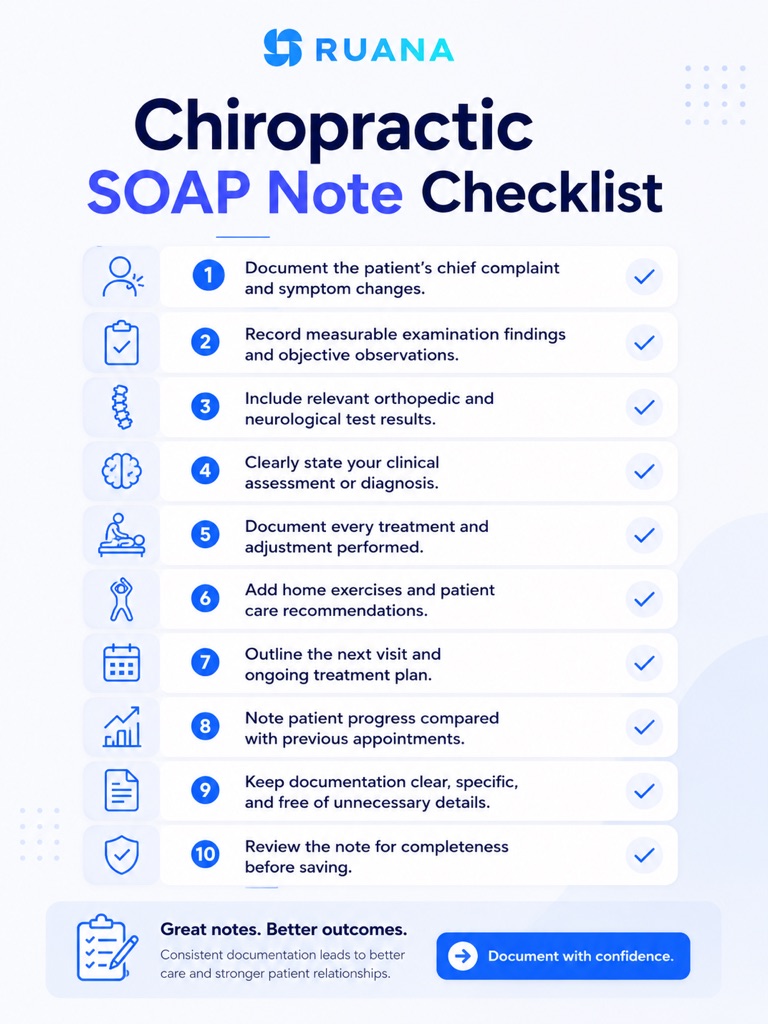
Chiropractic SOAP Note Checklist
Before signing off on a patient visit, take a moment to review your documentation. This quick checklist can help ensure your chiropractic SOAP notes are complete, consistent, and ready for future treatment, insurance reviews, or compliance audits.
Final Thoughts
Well-written chiropractic SOAP notes benefit everyone involved in the patient’s care. They provide a clear record of clinical findings, support better treatment decisions, simplify insurance documentation, and protect your practice when records are reviewed.
The key is consistency. Using a structured SOAP format and standardized documentation process allows chiropractors to maintain high-quality records without spending unnecessary time on paperwork.
Dedicated chiropractic practice management software can help you keep patient records, scheduling, charting, and SOAP notes connected in one workflow, making documentation faster and easier to manage as the practice grows.
What are the 4 components of a SOAP note?
A SOAP note consists of four sections:
Subjective, where the patient describes their symptoms.
Objective, which records measurable examination findings.
Assessment, containing the chiropractor’s clinical evaluation.
Plan, outlining the treatment provided and next steps in care.
How do chiropractors write SOAP notes faster?
Chiropractors can reduce documentation time by using standardized templates, documenting visits immediately after treatment, avoiding repetitive free-text entries, and using practice management software with built-in SOAP note workflows. This helps maintain consistency while reducing administrative work.
Can ChatGPT write SOAP notes for chiropractors?
ChatGPT can assist with drafting or organizing SOAP notes, but every note should be reviewed and completed by the treating chiropractor. Clinical findings, diagnoses, and treatment decisions must always reflect the patient’s actual examination and the practitioner’s professional judgment.
Can SOAP notes help with insurance claims?
Yes. Complete and accurate SOAP notes help demonstrate medical necessity, document patient progress, and support the treatments billed. Well-maintained documentation can also simplify claim submissions and provide valuable evidence during insurance audits or record reviews.
About the Authors
★★★★★4.9 · 329 Reviews
Rouzbeh NoroozyChiropractor & Co-Founder · Palmer West · UC Berkeley · 14 Years of ExperienceRouzbeh Noroozy is a chiropractor with 14 years of clinical experience and co-founder of Ruana practice management software. He completed his undergraduate studies at the University of California, Berkeley and graduated from the renowned Palmer College of Chiropractic West in California. As a practicing clinician and clinic owner, he understands firsthand the administrative challenges practices face — and which digital tools genuinely help streamline day-to-day operations.
Anastasiia NoroozyMedical Graduate & Co-Founder · 8 Years of ExperienceAnastasiia Noroozy is a medical graduate and co-founder of Ruana with 8 years of experience working directly with patients at the clinic in Cologne. She manages the day-to-day flow of the practice and knows every patient-facing process from the inside out — from intake and scheduling to follow-up care. Her hands-on clinical and operational experience directly shapes how Ruana is built to work in the real world.
Our team will review your inquiry and get back to you as soon as possible.
Privacy Settings
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Analytics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.
To provide the best experience for our practitioners, we use cookies to personalize content, analyze our traffic, and support our marketing efforts. By clicking 'Accept', you consent to our use of these technologies. You can manage your preferences at any time.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Analytics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.