Weak notes create strong problems. They slow down charting, make insurance support harder, and leave too much room for missing details.
That’s where a clear SOAP note system comes in. This guide breaks down exactly how to write SOAP notes that are fast, organized, clinically useful, and easier to defend when documentation needs to support continuity of care or reimbursement.
Massage therapy continues to serve a large health-focused audience. AMTA reports that 71% of massage consumers used massage for a health or medical reason in the 12 months ending June 2025, and 29% used it for pain relief or pain management.
Structured documentation also matters because SOAP notes are a widely used healthcare standard, and strong records help communicate what the patient reported, what you observed, how you interpreted it, and what you plan to do next.
Key takeaways
- SOAP stands for Subjective, Objective, Assessment, and Plan.
- Good SOAP notes connect symptoms, findings, treatment, and next steps in one clear clinical story.
- For massage therapists and chiropractors, the strongest notes include measurable findings, response to care, and a plan tied to the visit.
- Students can improve quickly by learning what questions belong under each SOAP section.
- Practice owners can save time with SOAP note templates and Advanced SOAP Notes inside Ruana.
Table of contents
What are SOAP notes and why do they matter? Subjective: what to ask and what belongs here Objective: what to measure, observe, and record Assessment: where clinical reasoning shows up Plan: what happens next and how to document it SOAP note question prompts for each section SOAP note example for massage therapy and chiropractic Common SOAP note mistakes that weaken your documentation How SOAP notes software makes charting faster SOAP notes: practical takeaways FAQWhat are SOAP notes and why do they matter for therapy practices?
SOAP notes are a structured clinical documentation format used across healthcare. They help you organize each visit into four parts: what the patient says, what you observe, how you interpret the visit, and what you plan next.
For massage therapists, chiropractors, and student clinicians, SOAP notes do more than keep records tidy. They help show medical necessity, support communication, reduce missed details, and create a timeline of progress from one visit to the next.
If you run a practice, good notes also protect your business. If you’re a student, they help you build strong habits before bad shortcuts become permanent. If you want software that supports both fast charting and organized records, explore Ruana’s practice management workflow and Ruana pricing and features.
Subjective: what to ask and what belongs in this section
The Subjective section captures what the patient reports. This includes symptoms, aggravating factors, relieving factors, functional complaints, and perceived changes since the last visit.
Think of Subjective as the patient’s voice inside the chart. You are not measuring here. You are documenting what the patient tells you in a clinically relevant way.
What belongs in Subjective
- Chief complaint
- Location of pain or tension
- Severity or pain rating
- Onset and duration
- Mechanism of injury or trigger
- Aggravating and relieving factors
- Functional limitations
- Changes since the last visit
- Patient goals
- Relevant home care compliance
Useful Subjective questions
- What brings you in today?
- Where exactly do you feel it?
- When did it start?
- Did it begin suddenly or gradually?
- How intense is it on a 0–10 scale?
- What makes it worse?
- What makes it better?
- Has it changed since your last visit?
- How is it affecting work, sleep, exercise, lifting, driving, or sitting?
- Have you tried anything at home since the last treatment?
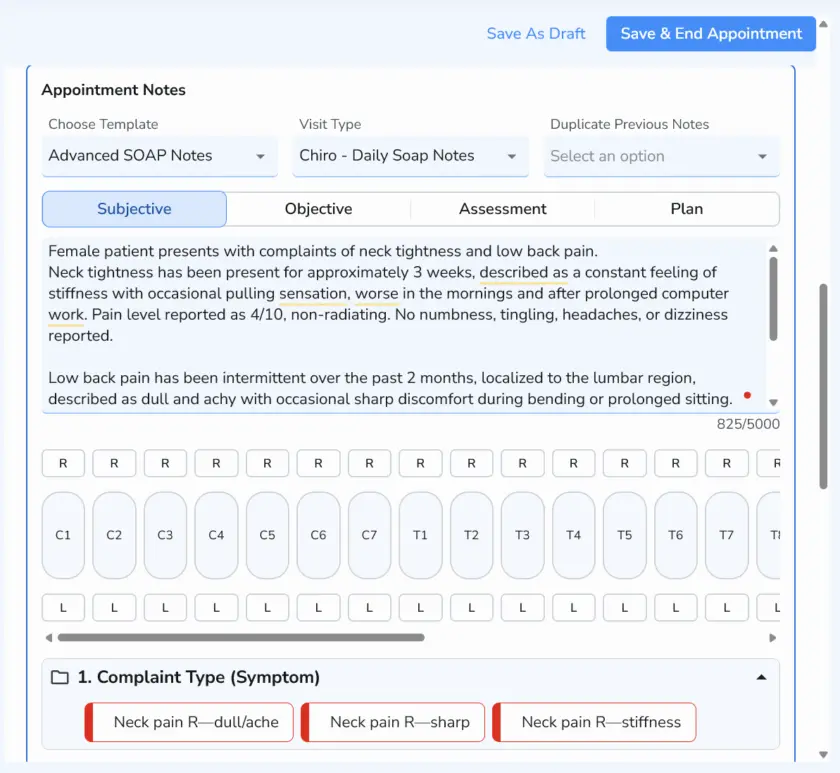
A strong Subjective section is specific. “Neck pain x 2 weeks, worse with rotation and desk work, 6/10 today, improved temporarily after last session” is far more useful than “neck still hurts.”
If your team charts the same subjective patterns all day, built-in templates can speed this up dramatically. That’s where Ruana’s SOAP Notes and Advanced SOAP Notes become practical, especially for repeat complaints and recurring visit types.
Objective: what to measure, observe, and record
The Objective section includes what you can see, test, measure, or palpate. This is where you document findings instead of opinions.
For massage therapists, this may include posture, tissue texture changes, tenderness, muscle guarding, range of motion, and treatment delivered. For chiropractors, it may also include segmental findings, orthopedic tests, neurologic observations, gait, and motion palpation findings when clinically appropriate.
| Objective item | Massage therapy examples | Chiropractic examples | Why it matters |
|---|---|---|---|
| Observation | Guarded shoulder posture, limited arm swing | Antalgic posture, pelvic tilt, head carriage | Shows visible dysfunction |
| Palpation | Hypertonicity upper trapezius, trigger points in levator scapulae | Paraspinal spasm, joint tenderness, myofascial restriction | Supports local tissue findings |
| Range of motion | Cervical rotation restricted bilaterally | Lumbar flexion limited with pain | Adds measurable comparison over time |
| Tests/measures | Pain scale, functional tolerance | Orthopedic or neurologic findings when relevant | Strengthens clinical support |
| Treatment provided | Myofascial release, trigger point therapy, stretching | Manual therapy, spinal adjustment, soft tissue work, rehab guidance | Documents what happened during the visit |
Questions that help you fill the Objective section
- What did I observe on arrival?
- What was measurable today?
- What findings were reproducible?
- What areas showed restriction, tenderness, or asymmetry?
- What treatment or intervention did I perform?
- How did the patient respond during and immediately after care?
Keep this section factual. “Upper trap hypertonicity noted bilaterally, left greater than right, cervical rotation limited approximately 15 degrees left with end-range discomfort” is objective. “Patient looked bad today” is not.
Assessment: where your clinical reasoning shows up
Assessment is where you interpret the visit. This is the part many students rush, but it is often the section that separates a weak note from a useful one.
Your Assessment should connect the Subjective and Objective sections. It answers the question: what do today’s findings mean?
What belongs in Assessment
- Your impression of the patient’s current status
- Progress, plateau, flare-up, or regression
- Tolerance to treatment
- Clinical response compared with prior visits
- Reasoning that supports ongoing care or a change in approach
Assessment prompts
- Is the patient improving, unchanged, or worsening?
- Did today’s findings support the patient’s complaint?
- How did the patient respond to treatment?
- What does today’s visit suggest about function or progress?
- Does the plan need to continue, progress, or change?
A good Assessment sounds like this: “Findings remain consistent with mechanical cervical dysfunction and myofascial restriction. Patient reports reduced headache frequency since last visit but continued pain with prolonged desk work. Tolerated manual therapy well with modest immediate increase in left rotation.”
That is concise, clinical, and connected. It shows judgment without becoming vague. If you want to make notes easier for your whole team to standardize, this is exactly where template-driven SOAP note software helps most.
Plan: what happens next and how to document it clearly
The Plan section records the next steps. It should make the follow-up strategy obvious to anyone reading the chart later.
This section can include the next visit frequency, home care, exercises, activity modifications, referrals, re-evaluation timing, or changes to treatment focus.
| Plan element | Examples | Why it strengthens the note |
|---|---|---|
| Frequency | Continue 2x/week for 2 weeks | Shows treatment structure |
| Home care | Pectoral stretch, hydration, ice/heat guidance | Demonstrates ongoing management |
| Next-session focus | Reassess cervical ROM and left upper trap tone | Creates continuity between visits |
| Referral/escalation | Monitor neurologic symptoms; refer if worsening | Shows judgment and safety awareness |
| Patient instruction | Avoid provocative lifting for 48 hours | Supports patient compliance |
Useful Plan questions
- When should the patient return?
- What should the patient do between visits?
- What will I reassess next time?
- What change in care is needed based on today’s findings?
- Does anything need referral, imaging, or additional follow-up?
The strongest Plan sections are specific. “Return next week” is weak. “Follow up in 5–7 days, continue home stretching twice daily, reassess cervical rotation and headache frequency, progress care if functional tolerance improves” is much better.
SOAP note question prompts for each section
If you want one practical trick that improves note quality immediately, it’s this: train yourself or your staff to think in questions. Good SOAP notes are easier to write when each section has its own prompt set.
Subjective prompts
- What is the patient feeling?
- What changed since last visit?
- What activity makes it worse?
- What does the patient want to improve?
Objective prompts
- What did I see, test, or measure?
- What tissues or joints were involved?
- What treatment did I perform today?
- What was the immediate response?
Assessment prompts
- What do today’s findings mean?
- Is the case progressing?
- Was today’s response expected?
- What supports continued care?
Plan prompts
- What happens next?
- What should the patient do at home?
- When should follow-up occur?
- What needs reassessment next visit?
These prompts are useful for solo practitioners, multi-provider clinics, and students still learning how to organize documentation. They also translate well into pre-built templates inside massage therapy software and chiropractic practice management software.
SOAP note example for massage therapy and chiropractic practices
Here is a simple example showing how the four sections work together.
S: Patient reports left-sided neck and upper trap pain for 10 days after increased desk work. Pain 6/10 today. Worse with turning head left and prolonged computer use. Mild temporary relief after prior massage. Sleep mildly disturbed.
O: Guarded cervical posture on arrival. Palpable hypertonicity left upper trapezius and levator scapulae. Cervical rotation decreased left with end-range discomfort. Manual soft tissue therapy, trigger point release, and stretching performed to cervical and upper thoracic region. Patient tolerated treatment well.
A: Findings consistent with mechanical cervical tension pattern and myofascial restriction, left greater than right. Functional irritation remains present with desk work, though patient reports slight short-term relief after previous care. Good tolerance to manual treatment suggests continued conservative care is appropriate.
P: Follow up in 5 days. Continue home pectoral and upper trap stretches twice daily, hydration, and workstation modification. Reassess cervical rotation and headache frequency next visit. Progress treatment plan if functional tolerance improves.
This example is simple, but it works. It tells a clear story, connects findings to care, and leaves the next provider or reviewer with a usable record.
Fast notes are useful only when they still show your thinking. The best SOAP note is not the longest one. It’s the one that clearly explains the visit.
Ruana documentation principleCommon SOAP note mistakes that weaken your documentation
Most SOAP note problems are not caused by a lack of knowledge. They come from rushed habits.
- Mixing sections together: putting opinions in Objective or findings in Subjective.
- Using vague language: words like “better,” “bad,” or “tight” without context.
- Skipping measurable findings: especially when range of motion, pain scale, or function can be tracked.
- Failing to show progress: a note should connect to the prior visit when relevant.
- Over-documenting irrelevant details: more words do not always mean better documentation.
- Copy-pasting without updating: this is one of the fastest ways to create weak charts.
Your note should help someone understand what happened, why it mattered, and what comes next. Anything that clouds that story weakens the chart.
How SOAP notes software makes charting faster for massage therapists and chiropractors
Once your note structure is solid, the next bottleneck is speed. That’s where SOAP notes software matters.
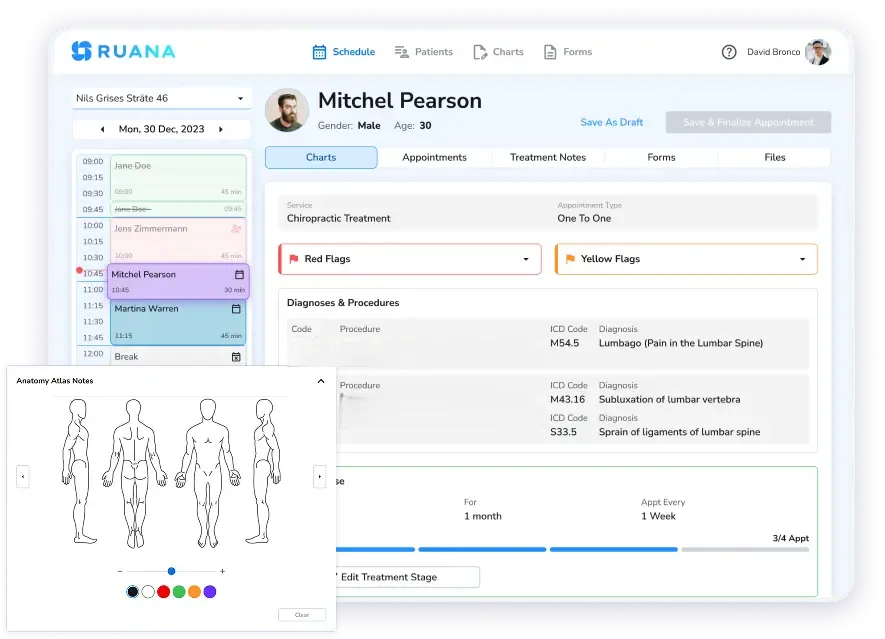
Ruana is built to help practices document faster with ready-made templates, customizable chart layouts, and Advanced SOAP Notes that let you insert full findings or treatment summaries with pre-programmed buttons. Ruana also supports scheduling, forms, billing, and reminders in the same workflow, so your note is not living in a separate disconnected tool.
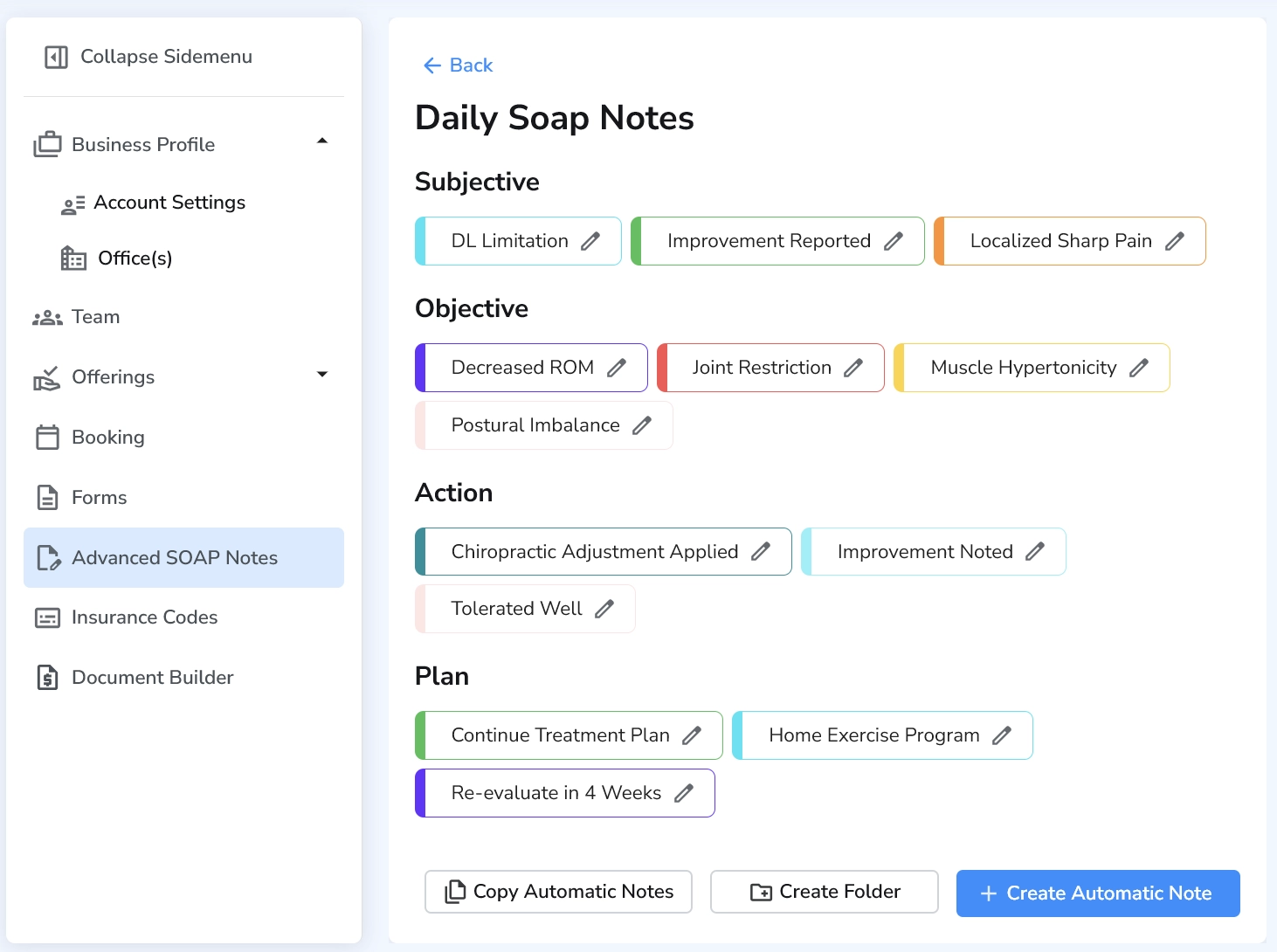
For students, software templates reinforce the right structure. For clinics, they improve consistency across providers. For owners, they reduce charting time without sacrificing documentation quality. See how it fits into massage therapy workflows and chiropractic practice workflows.
SOAP notes: Practical takeaways
- Use Subjective for what the patient reports, not what you measure.
- Use Objective for findings, tests, observations, and treatment delivered.
- Use Assessment to explain what the visit means clinically.
- Use Plan to show what happens next, including follow-up timing and home care.
- Ask repeatable questions under each section so charting becomes faster and more consistent.
- Track measurable change whenever possible, especially pain, function, tolerance, and ROM.
- Keep your notes relevant, concise, and specific enough to support continuity of care.
- Use SOAP notes software like Ruana’s charting tools if you want to reduce repetitive typing and standardize documentation across your practice.
Write better SOAP notes without slowing down your day
Ruana helps massage therapists, chiropractors, and growing practices chart faster with SOAP note templates, Advanced SOAP Notes, scheduling, reminders, forms, and billing in one workflow.
Try it free for 14 days with no credit card required and see how much faster your documentation can feel.
Try Ruana FreeFAQ
What does SOAP stand for in SOAP notes?
How do massage therapists write SOAP notes?
How do chiropractors write SOAP notes for insurance support?
What should go in the Assessment section of a SOAP note?
What are common mistakes when writing SOAP notes?
Can students use SOAP note templates to learn faster?
What is the best SOAP notes software for massage therapists or chiropractors?
Do SOAP notes need to be long to be good?
This article is educational and should be adapted to your jurisdiction, payer requirements, licensing rules, and scope of practice.